First, this information proves that legitimate opioid prescriptions are not the CAUSE of our current fake “opioid crisis”, but simply a means to attack physicians for money to pay government agents. It has been going on for years before the increase in treating pain. Second, I will use their data to explain drug addiction through the REAL cause.
Findings From the Study.
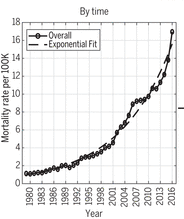 The overall mortality rate for unintentional drug overdoses in the United States grew exponentially from 1979 through 2016 along a remarkably smooth trajectory. But trajectories of deaths from individual drugs have not tracked along exponential trajectories. Cocaine was a leading cause in 2005–2006. Then came prescription opioids, then heroin, and then synthetic opioids such as fentanyl.
The overall mortality rate for unintentional drug overdoses in the United States grew exponentially from 1979 through 2016 along a remarkably smooth trajectory. But trajectories of deaths from individual drugs have not tracked along exponential trajectories. Cocaine was a leading cause in 2005–2006. Then came prescription opioids, then heroin, and then synthetic opioids such as fentanyl.
The demographic patterns of deaths due to each drug have also shown substantial variability over time. Until 2010, most deaths were in 40- to 50-year-old persons, from cocaine and increasingly from prescription drugs. Deaths from heroin and then fentanyl have subsequently predominated, affecting younger persons, ages 20 to 40. Mortality rates for males have exceeded those for females for all drugs. Rates for whites exceeded those for blacks for all opioids, but rates were much greater among blacks for cocaine. Death rates for prescription drugs were greater for rural than urban populations.
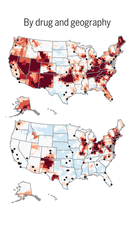 The geographic patterns of deaths also vary by drug. Prescription opioid deaths are widespread across the United States, whereas heroin and fentanyl deaths are predominantly located in the northeastern United States and methamphetamine deaths in the southwestern United States. Cocaine deaths tend to be associated with urban centers.
The geographic patterns of deaths also vary by drug. Prescription opioid deaths are widespread across the United States, whereas heroin and fentanyl deaths are predominantly located in the northeastern United States and methamphetamine deaths in the southwestern United States. Cocaine deaths tend to be associated with urban centers.
Conclusion
According to the authors, this historical pattern of predictable growth for at least 38 years suggests that the current opioid epidemic may be a more recent manifestation of an ongoing longer-term process. [Really? No duh!!] This process may continue along this path for several more years into the future. Paradoxically, there has been substantial variability with which specific drugs have become dominant in varying populations and geographic locales. This variability all but negates the possibility of confident predictions about the future role of specific drugs. Indeed, it is possible that a future overdose epidemic may be driven by a new or obscure drug that is not among the leading causes of drug overdose death today. Understanding the forces that are holding multiple subepidemics together onto a smooth exponential trajectory may be important in revealing, and effectively dealing with, the root causes of the epidemic.
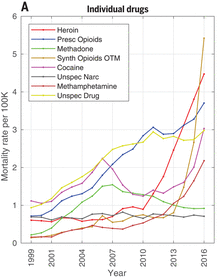 Detailed data for individual drugs are only available from 1999 to 2016, although additional data for all drugs are available since 1979. Since 2010, the mortality curves for all drug types have been increasing, except for methadone and for unspecified drugs and narcotics. The mortality rate from prescription opioids decreased slightly in 2012, whereas the mortality rates from heroin and synthetic opioids have been increasing rapidly. These trends are probably related because of the government interference in prescriptions forcing patients to switch to illicit opioids. Economic factors may also have contributed since heroin is increasingly more available, easier to use through non-oral routes, and becoming purer and less expensive than prescription opioids.
Detailed data for individual drugs are only available from 1999 to 2016, although additional data for all drugs are available since 1979. Since 2010, the mortality curves for all drug types have been increasing, except for methadone and for unspecified drugs and narcotics. The mortality rate from prescription opioids decreased slightly in 2012, whereas the mortality rates from heroin and synthetic opioids have been increasing rapidly. These trends are probably related because of the government interference in prescriptions forcing patients to switch to illicit opioids. Economic factors may also have contributed since heroin is increasingly more available, easier to use through non-oral routes, and becoming purer and less expensive than prescription opioids.
Patterns Identified:
- A clear bimodal distribution of unintentional drug overdoses: a younger group (age 20 to 40 years) due to heroin and synthetic opioids among males, whites, and in urban counties and an older group (age 40 to 60 years) from prescription opioids and unspecified drugs among females, whites, and in rural counties.
Part of the problem with their blaming prescription drugs on deaths today is that overdose deaths prior to 1999 were not attributed to prescription opioids owing to lack of toxicology testing for drug specificity, so were just listed as “unspecified”. However, the patterns of overdose mortality rates for which the drug was unspecified closely resemble the patterns for prescription opioids across age, gender, race, and urbanicity. And back in 1979, most of the drugs now being blamed for the “epidemic” didn’t even exist.
Mortality differences between male and female rate are associated with age and type of drug. Prior reports of prescription opioid mortality rates have shown nearly four times higher rates in younger males than younger females, in contrast to only 1.3-fold higher rates in older males relative to older females, most likely explained by the type of drug. The higher risk among young males relative to young females is mostly attributable to heroin and synthetic drugs, whereas the risk of death among older females is mostly attributable to prescription opioids and unspecified drugs. These differences by age, sex, and type of drug have generally become more apparent in recent years.
The association between drug overdose deaths and race in the literature has been mostly limited to reports that show increased mortality rates, especially for opioids among whites. The peak mortality rate for cocaine among blacks has increased with each year, especially among men and in urban counties. Among whites, the younger age group is at greatest risk for heroin and synthetic opioid deaths, whereas among blacks, the older age group is at greater risk.
The increase in mortality in 2016 is due to multiple drug-specific subepidemics: synthetic opioids (most likely fentanyl) among males, whites, and those in urban counties; heroin among young adults; prescription opioids among the middle-aged and blacks; and cocaine and methamphetamine among a wider age range, males, and whites.
Geographic hotspots of each of the drugs from 1999 to 2016 shows that, although the overall national epidemic may be smooth and continuous, each drug has shown a specific geospatial pattern of spread. Heroin hotspots have changed from being closely clustered around large cities to being distributed more widely, especially in the Northeast and the Southwest. Prescription opioid hotspots initially were prominent in the southwestern United States and Appalachia but subsequently spread to involve much of the western United States, Oklahoma, Florida, and New England. Fentanyl and fentanyl analog hotspots have centered in opioid hotspots, especially in the Appalachian and Northeast regions. Cocaine hotspots have also centered around large cities but have diffused more broadly in recent years. Methamphetamine deaths have increased most dramatically in the western and southwestern United States Almost every region in the country is a hotspot for mortality from one or more drugs. The only large region that appears to have been relatively spared (a relative “cold spot” for all drugs) is composed of the north central states.
The researchers can’t put it all together as to mechanisms of cause. But they do recognize that the current “opioid crisis” may be part of a larger, longer-term process. The epidemic of drug overdoses in the United States has been inexorably tracking along an exponential growth curve since at least 1979, well before the surge in opioid prescribing in the mid-1990s. This historical pattern of predictable growth for at least 38 years strongly suggests that the epidemic will continue along this path for several more years.
Now for my interpretation
Throughout history there has been a recognized 1% of the population who have been “addicted” to a drug, primarily alcohol, even though opiates were available OTC. Then, as described in my DVD on the REAL Cause of Drug Abuse, in 1869 Dr. George Beard proposed his theory of neurasthenia, which he attributed to modern civilization. Since the 1950s, modern civilization has intensified. Healthy habits have been replaced by unhealthy ones.
I attribute the increase in addiction today (which is probably up ½% from 100 years ago,) to:
- 1950’s: Overuse of antibiotics destroying our natural microbiome.
- 1970: Invention of HFCS (high fructose corn syrup) and the following increase in carbonated beverage consumption, increasing acidity in the diet.
- Increase in processed and fast foods that are sugar-high, toxin-high, and nutrition-low.
- 1980’s: Overuse of vaccinations, especially for non-life-threatening diseases, and with completely unnatural, man-made substances.
- 1990’s: Invention of Roundup Ready and the development of GMO’s allowing it to be sprayed on all of our most consumed foods, also destroying our gut microbiome.
None of this has to do with prescription opioids, except for the fact that they are available and they relieve the addict’s anxiety caused by the toxicity. But charging doctors for crimes for prescribing them and continuing the archaic, racist-based attacks on drugs themselves is completely asinine. But until the American people learn the truth, which is found on this website, the direction we are heading will not change. That is because conventional medicine has no clue what causes addiction. The answer is found in my DVD, The REAL Cause of Drug Abuse.
Join us in this fight today. Get your own copy and spread the word.
Linda Cheek is a teacher and disenfranchised medical doctor, turned activist, author, and speaker. A victim of prosecutorial misconduct and outright law-breaking of the government agencies DEA, DHHS, and DOJ, she hopes to be a part of exonerating all doctors illegally attacked through the Controlled Substance Act. She holds the key to success, as she can offset the government propaganda that drugs cause addiction with the truth: The REAL Cause of Drug Abuse.
Get a free gift to learn how the government is breaking the law to attack your doctor: Click here to get my free gift